

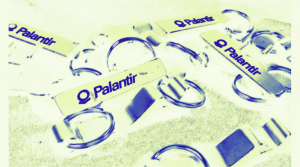
© Steve Eason/Flickr
The legacy of the junior doctors’ strike
Ian Allinson •Ian Allinson, a recent challenger in Unite the Union’s general secretary election, interviewed Emma Runswick, a key organiser around the dispute in Manchester and a medical student active in both the British Medical Association (BMA) and ‘Doctors in Unite’ about what happened and the how it changed organisation inside the NHS. Photos by Steve Eason.
This interview was originally published in rs21’s magazine. To buy the full issue, click here.
Ian: As a medical student, how easy was it to get involved in the Junior Doctor’s strike?
Emma: Relatively easy. The Junior Doctor’s strike was quite strange in a number of ways, in that the BMA held back from doing a lot of the groundwork early on. So the early demonstrations, both the one in Manchester and the one in London outside NHS employers’ events were actually organised by medical students. The NHS held events all over the country, or more accurately, they were supposed to hold events all over the country. We organised demonstrations outside for people who could not get in including medical students and huge numbers of doctors.
In Manchester, it was organised by myself and Zoe Brunswick who is a member of the Socialist Party and was the BMA rep for medical students at the time. In London, it was organised by people involved in the Docs Not Cops movement, an organisation that organises against borders enforcement in the NHS.
Ian: Why do you think the students ended up playing such a prominent role?
Emma: From very early on, I think it was because we had a lot more time than doctors did. Doctors were trying to organise to go to these kinds of events; the reps were often working hard to get people to vote yes in the ballot. At that point the BMA wasn’t doing very well at responding to events, so when NHS Employers said they were going to put on meetings, there was a very confused response about what BMA members should go, whether they should go and walk out, whether they should go and ask questions. For those of us who had a background in activism, it was much more straightforward– hold a demonstration, use shouts like “They can’t lie to you”.
So quite early on, it was easy to do that kind of work. It was relatively easy to produce your own leaflets and placards because the BMA leaflets were very poor. They sent some to the demonstration in Manchester, which were A4 black and white information sheets about why we oppose all the clauses in the contract, which was not what we needed at all. We were trying to leaflet the public about why we were there, why doctors were going on strike and so on. So initially, it was super easy to get involved in the strike.
As it went on, it became more difficult to get involved because it was not a medical students’ strike. There was some efforts, mainly from anarchist and revolutionary socialists who were medical students to get a medical students’ strike to take off, but it didn’t really get anywhere, though we were reasonably successfully organising medical students to join the pickets, even if only for a short period of time. However, primarily it was the doctors’ thing, and that was how it should have been.
Ian: So can you briefly remind people what happened with the Junior Doctors’ strike?
Emma: So we were in negotiations over a new contract for a long, long time, probably two or three years before 2015, recognising that there were problems with the old contract as well. The Department of Health and the government had a desire to get rid of our unsocial hours, to make it much cheaper to employ us on evenings, weekends, to attack pay progression – very similar things to what they are doing in the rest of the public sector to be honest.
Eventually we withdrew from negotiations, as we were not getting anywhere, none of our problems were being solved, and it was quite clearly just an attack on our terms, conditions, and pay. We opened a ballot for strike action in November 2015. This was over two weeks and when it came back, there was a big campaign to get people to vote and to vote yes, it came back with 76% turnout, 99.4% yes for action short of strike, 98% in favour of strike action. One of the best days of my life so far. The moment when you realise “Wow that is massive”. It was massive. There we were, going out on demonstrations, organising pickets, although at that point, it was very difficult to organise pickets, actually.
Ian: To take you back a step, what was the organisation like before the strike to deliver that vote?
Emma: Very poor. We do not have a layer of activists in the BMA, really. This has changed to a certain extent now but then we mainly had people involved in the BMA for career reasons, in the professional association side or people who liked the scientific work that the BMA did. We also had a number of people who are interested in medical politics but very little rank and file organisation. We did not have any lay reps who do case work, that is all dealt with by staff members, so there was very little going on.

© Steve Eason/Flickr
A number of things created the vote. First, the outrageousness of the contract. People read it or read parts of it and were beyond shocked. And this was actually expressed in interesting ways by Conservative voting doctors who were shocked that they could be treated like this, as professionals, how could this happen? So first, it was just so awful, and everybody could see it.
There was a reasonable campaign by Junior Doctors, both people who had been involved in negotiations and people on the left. There was an excellent social media element. We were developing Junior Doctors’ contract forums, many people were sharing things, and there was a big encouragement to vote yes.
Ian: After the vote, it seemed to take off, people were inspired by this group of people who often hadn’t seen themselves as workers, had been traditionally quite conservative, having these big lively pickets, with young people involved and so on. The strike seemed to go through a number of stages and then fizzle out. So what happened with the strike once it was underway?
Emma: First, we called strike action and cancelled it several times, due to various promises from the government. So we had a bit of a stuttering start, which at the time I found both very frustrating but actually was quite useful because we did not have the organisations to bring out as many people as we did when we first announced that strike action, or to organise effective pickets or even just numerous pickets.
However, we had a series of strike days, starting with emergency care only, and then moving into all-out strike action. There was a lot of disagreement about whether that was appropriate. There were many people who were in favour of strike action, but only if it did not affect patients. That is quite a strange situation to be in if your work is treating patients, that you draw the line at all-out strike action, still going in to do on-calls and emergency cover.
So we had a period where people who were working in routine work, so not emergency medical cover and not in A&E, people doing routine jobs would come out, but people in emergency would not, and then you had everybody, all junior doctors regardless of what they would doing coming out. The impact of those strikes were really massive, we had multiple reviewed offers, each one was better than the last though if you compare the contract which has been imposed to the one we were originally offered when we balloted to strike you really can see the difference that the strike action made.
Nevertheless, eventually one of the offers was put to a referendum and the chair of the Junior Doctors’ Committee at the time was very much in favour of it. He said it was a good contract. The BMA was officially neutral. Those of us on the left campaigned for a rejection. We thought it still was very poor, particularly for less than full-time workers, predominantly women and disabled people, and that it was insufficient to protect evenings and weekends, so we campaigned for a rejection and won with 58% of the vote. The chair of the JDC who had been in favour of the contract, stepped down, and Ellen [McCourt] was elected in his place.
The JDC called a survey to try to understand why people rejected the deal. The survey then took a while, not huge numbers participated in it, certainly not in the numbers that had participated in the ballot and the referendum, but because we had had a break in the momentum of the dispute, there was increasing disquiet among members. Many people were frustrated that we needed to be a survey. I think there was a lot of legitimate criticism made of BMA communications in this time, but also a lot of misunderstanding about what was happening internally because many of the delays were political fights really, about what we should do next.

© Steve Eason/Flickr
After a long period of doing nothing, and a very split result in the referendum, that announcement of further strike action was received very badly. It was certainly received very badly by the press, many groups, such as senior doctors, who had previously supported the dispute, did not support it anymore, and there was a very mixed response from members. Even those who very in favour of putting forward a model contract and not accepting any detriment to our conditions did not feel those five days were appropriate.
At that point, it began to fall apart. There were many internal attacks. The previously very communal atmosphere, everybody was in it together, fell apart. A number of things happened and the first five days of strike action were cancelled. Partially, that was because the NHS said they would not be able to be safe. There was some indication that they would hold junior doctors who were on strike responsible for any harm caused during the strike days, and would report people to the professional regulators. Once that first five days was cancelled, it became difficult for the BMA to continue with the five days further down the line.
After that, there was no further action, and the contract began to be imposed in October, it was imposed on the first set of doctors in October. From that, point there is very little good really. The JDC became very toxic, Ellen resigned, and her deputy chair stepped up but did not want to re-stand and at that meeting nobody stood so the new deputy chairs stepped in to again be interim chairs for a bit.
Nobody really knew how to deal with the problem that we now had, and it became very, very difficult. Huge numbers of members felt that they had been sold out; though I think, it is far more complicated than a sell-out in the way that you see in the pension’s dispute for example. It is more that it all went wrong, rather than they made a conscious decision to sell out.
Now, moving forward, we want to try to use the good parts of the contract. Particularly we want people to use the exception reporting system in the contract, which allows you to get pay or time off in lieu for extra hours or deviations from your rota. We have a review coming up of the contract in 2018 which, at the junior doctors’ conference this year we secured a ballot [on the proposal], or a referendum, so whatever the result of that review is, there will be a new opportunity for further action.
Ian: So from that whole process what were the most important things you learned?
Emma: That you often have to do it yourself. There is a lot of criticism made of many big trade unions but the BMA really was not prepared for this. It was not prepared as an organisation. It was not ready on the ground for this level of industrial action, and that meant that often we needed to do things ourselves.
We produced leaflets ourselves, we produced our own banners, the North West regional BMA banner was painted by me and some comrades in Manchester students’ union one afternoon and I am very proud of it but it is not like a branch banner you would expect in another union. A junior doctor in London produced the posters that went up in thousands of houses. She contacted the CWU who agreed to distribute some, and sent them out to other trade unionists and to other individuals who went round their town centres and asked people to put them up in their shop windows and so on. The demonstrations, certainly initially, were organised by just activists, often not in any way associated with the BMA apart from being members.
So that is the first thing – you often have to do it myself. The aim of course is to get to the position where you do not have to do it yourself where it is the union that is doing those jobs, and in many things, we did get to that point during the course of the dispute. The demonstrations are a good example of that. Also, the way in which it moved from being, whenever they wanted to interview somebody just anyone available would do it, then towards the end the BMA had trained more people to deal with the media.

© Steve Eason/Flickr
Ian: There was support from outside the BMA for the dispute. You have mentioned the CWU helping with distributing posters, and obviously the medical students’ role. More generally, what impact do you think solidarity from outside had on the strike?
Emma: The impact of patients’ support was massive. The fact that patients came to picket lines, delivered food, wrote letters, rang into radio stations, supported people on Question Time and everything, and had a massive impact on morale. Kept the strike going when people were finding it difficult. That was primarily because the view of the profession is that we are there for patients, and the criticisms that the Tories made that we were putting patients at risk and so on were pushed back by the support that we had from patients.
There was also considerable support from the trade union movement, but I think it was very instructive for lots of people who had not previously considered themselves workers, had not considered themselves part of the trade union movement. At the beginning of the dispute a comrade of mine in the BMA posted in the Junior Doctors’ Contract Forum’ Facebook group with 54,000 Doctors and medical students in it, an article about an RMT dispute that was happening around the night-tube. People responded by going “this is nothing to do with us”, “why should we care about these people, they’re only going to make our days really difficult, they’re money grabbers” and so on.
Several months later, the attitude had completely changed. When someone else posted about it, people were drawing comparison, like well they’re being told they have to work more hours for no extra pay, they haven’t got appropriate safety considerations and so on, and that change I think came from the support we got from people.
The BMA would not do it, would not contact other trade unions, or at least would not ask for help, it would not set up a Skype call or anything, so it was done on a very ad hoc basis. In Manchester, we got a lot of support from the trade union council, in London, the RMT were very very supportive and also the teachers. The NUT were going through a dispute around academisation, and the London regional Junior Doctors’ Committees and the NUT managed to hold a joint demonstration which they brought Jeremy Corbyn and John McDonnell to speak at.
There were regularly people from other trade unions on our picket lines coming to speak to strikers. I don’t think it impact on morale in the same way that patient input did, but it did impact on the way that people saw themselves and the way they saw the strike because they got assistance and support from people in the trade union movement – other workers, workers who often were poorer than them. They did not get support from places they expected to get support, from the press, from their local politician, particularly Conservatives found themselves quickly disillusioned with the idea that their politicians spoke for them. So I think it was very important for a shift in very many doctors’ heads of trade union consciousness and political orientation.
Ian: Just going back to the strike itself, what would it have taken for a clearer win as members saw it, in terms of the politics or the organisation of the BMA?
Emma: I think we would have needed a much stronger rank and file, an organisation of members and activists that were ready for that level of a dispute. I do not think that would have been possible without having one of these kinds of disputes, so it is something of a circular argument. I think we needed people on the JDC and other committees in the BMA to have much better mechanisms for understanding what was going on the ground. So we had lots of online activity, we had lots of surveys, we had emails, we had social media, but we didn’t have the kind of knowing who people were in every hospital and how many members we had, what the turnout was likely to be.
Because of that, a lot of decisions that we made, and a lot of the opinions that were formed, and not just on the JDC but among the broader membership, was based on what they saw in social media and in the press. So when the press turned against us, they found that very difficult to maintain. When they found they were hearing from Johann that it was a good contact and their members still rejected it, they did not understand why. I think that is again a failure to have rank and file organisation and a good communication between national committees, reps and ordinary members.
But I think we still haven’t got that [rank and file], there’s still a big disconnect and that’s partially maintained by the fact that we don’t publish agendas, or minutes, or voting records and so on. The toxicity and the abuse that people got as it all fell apart has really caused that. There is an unwillingness to share with ordinary members what is happening and I think that can only lead to further failure.
Ian: You mentioned the pressure for more democracy and transparency in the BMA. People often see the mainstream unions as fairly inhospitable to radical or grassroots activism. Can you say a bit more about the barriers you face in the BMA and how you are trying to surmount them?
Emma: The BMA is quite a strange union. It represents a professional group who do not see themselves as workers. We also represent plenty of people who are not just workers in a Marxist sense, certainly. GPs are part self-employed, or running small businesses. Many people are involved in private practice. We have a quite strange make-up of better off workers and small business owners. There is a strong history of the BMA being very small ‘c’ conservative. It sees itself as a lobby group, a professional association and for a long time it had a separate organisation it had set up if it was going to take industrial action, so the BMA did not call any action, the British Medical Guild did. Even though it was obviously the same group.

Emma speaking at a conference in Manchester in 2015
So you have a historical weirdness going on. Many members are very reluctant to be seen as political. I mean, we describe ourselves as an apolitical trade union and professional association, so reaching out to politicians on a non-partisan basis is something we do regularly in lobbying but actively asking the TUC or the Labour Party and so on to support actions taken demonstrations or whatever, is quite difficult.
It is quite opaque and I do not think this is particularly unique to the BMA, I know it happens in other unions where there are not any minutes available to members, and it is difficult to find out how your representatives voted. It is my opinion that the staff of the BMA have quite a lot of power; a lot of the work is done by them rather than by elected representatives or trade union officials.
It is quite a strange place to be a trade unionist but groups like Doctors Represent aim to help activists to organise – that is what we are here for. We want there to be rank and file organisation in every hospital, every GP practice, in public health sections, everywhere. We want that to be the basis of our industrial strategy both on a very minor level as in a small rota issue problem where all of you just refuse to cover the gap so they just have to hire someone else, all the way up to national disputes like the contract.
Ian: You talked about finding and identifying new activists before. Are there meetings happening in hospitals where people can discuss stuff and new activists emerge? How do you go about finding new people?
Emma: In some places there are hospital meetings – not many but in some. There are local negotiating committee meetings, but not everyone goes to those, you have to go through training to get onto one of those committees, not every hospital will have a junior representative on those.
The BMA operates on a divisional level, so that’s all branches of practice in a reasonably small geographical area like Manchester and Salford, and then a regional area which is on a branch of practice basis, so junior doctors in the North West region for example, or in the Thames region, and these regions are on the basis of how many people are in them. Attendance varies massively; some places have six people turn up, some places 60 turn up. During the strike, these meetings would have hundreds turn up. We picked up people there who wanted to do things.
Now a lot of recruiting of activists is done on a one to one basis. Somebody who has a problem or is angry about something and is willing to do something, and also people who come to national BMA events like student conference or the junior members forum. People who have nobody nearby who they can talk to about getting involved can apply to come to an open BMA event and meet other people there who will help them get active.
In some areas they’ve started these pilot things where you don’t have to be a rep, you just sign up to be a member volunteer and I don’t know a huge amount about how successful those have been or what member volunteers are doing in the areas where they’ve piloted it. But it seems to be associated with extra staff resources so we will see how that goes.
Ian: Obviously many of the battles going on are quite defensive because of all those cuts but if we had a big social change how would you envisage a socialist health care system?
Emma: We would have a huge amount of investment in public health. There are many conditions that we used to have in the UK, which we do not have anymore, particularly in terms of infection, because of improved water supply and so on, changes in industrial conditions. What we now need to get rid of is the factors that make people ill, like tobacco, alcohol, obesity. These are all areas where it is in capitalism’s interest to make us ill. Those industries – food, alcohol, tobacco – kill us and they disproportionately kill poorer people at ridiculously high rates. If we had proper investment in public health, proper regulation of these things then the country’s health would be a lot better, and there’d be less need, actually – if you talk about reducing demand, normally when Tory politicians talk about reducing demand they mean preventing people who need health care getting health care but in a socialist world we would genuinely have less need for health care.
We would have real public transport and work closer to where we live, we would work less, we would work nicer jobs, and the health service we would be fully staffed. We would have decent pay and conditions for all staff, not just doctors but health care assistants, cleaners. There is a big strike, or an important dispute, going on now at Bart’s Trust where many of those ancillary staff have been outsourced to Serco. They have been treated disgracefully. None of that in a socialist health care system.
I would like to see a salaried GP service. This is very contentious among GPs who do not want to be employed by the government because the government are awful, and they do not want to see a loss of independent practice, but I think that is the way forward. Increasingly people are salaried GPs anyway; no one wants to do the management work of a GP practice.
Ian: You make it sound as if a lot of the resistance to working for the government is because of that feeling that the government does things you do not agree with. I guess a question would be how decisions would be made in a socialist health care system. How would the people who worked in it, or the patients and the community, be in control of it in a democratic way?
Emma: One of the reasons I am involved in Doctors in Unite is that it is doing some great work on this actually. We have a document called Vision for the NHS, which discusses how neighbourhood health trusts comprising patients and health care workers could decide what was necessary for their communities, and you would build up from that basis. Reclaiming the word ‘commissioning’ away from what commissioning means now which is having a purchaser/ provider split and getting private companies to do the work for you towards what commissioning really means which is planning. So that workers and patients have joint say in the services that are delivered.
Ian: What do you see as the next steps in the defence of the NHS?
Emma: I think the Scrap the Cap campaign is something that we should really keep an eye on. The Royal College of Nursing said that if the government did not change their policy, that they would be balloting for strike action. It remains to be seen whether that will hold. There are certainly lots of good activists in the RCN who are doing good work in that union trying to get them to fight for their members, and not just for their members but for all public sector workers. I think that is something we should keep an eye on.




0 comments